

Whiplash Associated Disorder (WAD) symptoms can fluctuate, span multiple systems, and be difficult to measure consistently over time. That makes both treatment and documentation challenging, especially when progress needs to be clearly demonstrated. This guide breaks down WAD, how it’s classified, and how clinicians can better evaluate and track recovery.
What is Whiplash Associated Disorder?
Whiplash Associated Disorder (WAD) is a group of symptoms that develop after acceleration-deceleration injuries, most often from car accidents. Most whiplash cases aren’t straightforward: symptoms can fluctuate, span multiple systems, and be difficult to measure consistently over time. That makes both treatment and documentation challenging, especially when progress needs to be clearly demonstrated. This guide breaks down Whiplash Associated Disorder (WAD), how it’s classified, and how clinicians can better evaluate and track recovery.
For a refresher our on-demand WAD neck pain webinar reviews practical evaluation and care considerations.
Whiplash associated disorder is frequently linked to motor vehicle accidents. Because symptoms can be variable—and care may intersect with insurance or legal documentation—clinics benefit from a consistent evaluation baseline and clear, repeatable progress tracking over the full episode of care. BTE’s approach supports clinicians with objective data capture and reporting so documentation can reflect both the patient’s starting point and measurable change over time.
How WAD is Classified (Quebec Task Force System)
WAD is a medical condition that goes beyond neck pain or stiffness. “Whiplash” describes the injury mechanism—rapid acceleration-deceleration forces that cause the head and neck to move like a whip. WAD describes the symptoms and functional problems that may develop after this injury.
The Quebec Task Force created the international classification system for WAD. This system divides injuries into five grades based on symptom severity and clinical findings. The classification guides treatment decisions and helps predict recovery outcomes.
The following table outlines the Quebec Task Force WAD classification system:
| WAD Grade | Symptom Presentation | Severity Level | Typical Care Approach | Prognosis Indicator |
|---|---|---|---|---|
| Grade 0 | No neck symptoms or physical signs | No injury | No treatment required | Complete recovery |
| Grade I | Neck pain, stiffness, tenderness only | Mild | Early active care, education | Excellent recovery (days to weeks) |
| Grade II | Grade I symptoms plus musculoskeletal signs (reduced range of motion, point tenderness) | Moderate | Multimodal therapy, active rehabilitation | Good recovery (weeks to months) |
| Grade III | Grade II symptoms plus neurological signs (decreased reflexes, weakness, sensory deficits) | Moderate-Severe | Comprehensive rehabilitation, specialist care | Variable recovery (months) |
| Grade IV | Grade III symptoms plus fracture or dislocation | Severe | Immediate medical intervention, surgical evaluation | Extended recovery (months to years) |
Who Gets WAD and When It Occurs
WAD affects 3-6 people per 1,000 population each year. It occurs most often in people aged 20-40 years. Women develop WAD more frequently than men, possibly due to differences in neck muscle structure and cervical spine anatomy.1
The acceleration-deceleration mechanism can happen in car accidents, sports injuries, falls, and workplace incidents. WAD severity does not always match the force of impact. Individual factors like pre-existing conditions, age, and psychological state affect symptom development.
How WAD Symptoms Present in Patients
WAD causes symptoms that affect multiple body systems. Recognizing the full range of symptoms helps people identify the condition and get medical care.
Physical Symptoms
The most common physical signs of WAD include:
- Neck pain and stiffness: Often the main complaint, ranging from mild discomfort to severe, disabling pain
- Reduced range of motion: Difficulty turning the head or looking up and down
- Headaches: Often start at the base of the skull and move forward
- Shoulder and upper back pain: May spread into the arms and hands
- Muscle spasms: Involuntary contractions in neck and shoulder muscles
Some patients also report jaw pain or clenching that can complicate headache patterns; our quick overview on TMJ disorders can help your clinicians screen and plan appropriate interventions.
Neurological Symptoms
WAD can affect the nervous system, causing:
- Tingling or numbness: Often in the arms, hands, or fingers
- Dizziness or vertigo: Balance problems and spatial disorientation
- Visual disturbances: Blurred vision or difficulty focusing
- Tinnitus: Ringing or buzzing in the ears
- Sensitivity to light and sound: Increased discomfort in bright or noisy environments
Cognitive and Psychological Symptoms
Many people with WAD experience:
- Sleep disturbances: Difficulty falling asleep or staying asleep
- Concentration problems: Reduced ability to focus on tasks
- Memory issues: Difficulty remembering information or events
- Irritability and mood changes: Increased emotional sensitivity
- Fatigue: Persistent tiredness despite adequate rest
When Symptoms Appear and Warning Signs
WAD symptoms may appear immediately after injury or develop gradually over 12-48 hours. This delayed onset is normal and occurs due to inflammation and muscle guarding responses.
Get immediate medical attention for:
- Severe neurological symptoms (significant weakness, numbness)
- Signs of spinal cord injury (loss of bowel/bladder control)
- Severe headache with neck stiffness
- Difficulty swallowing or speaking
- Loss of consciousness or confusion
How Objective Measurement Makes a Difference in WAD
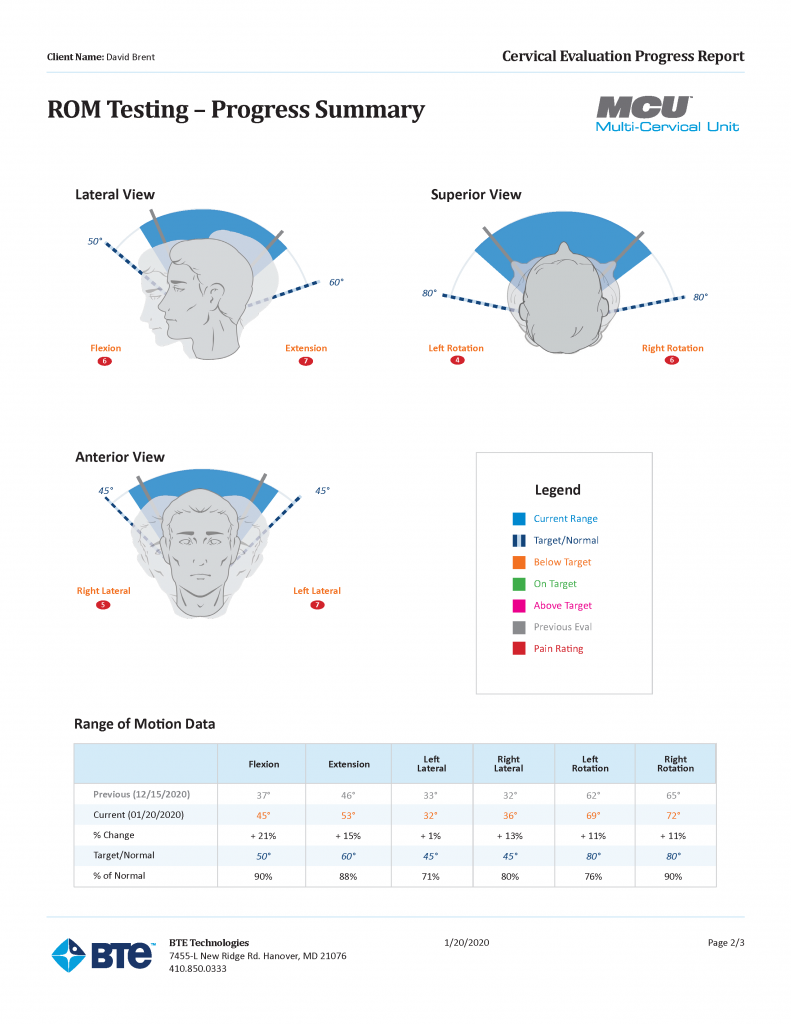
In whiplash cases, subjective findings alone often fail to clearly document what’s changed between evaluation, re-evaluation, and discharge—especially when patients report fluctuating pain, dizziness, or activity tolerance. Using objective measurements helps clinicians document deficits and progress in a way that’s easier to understand and share.
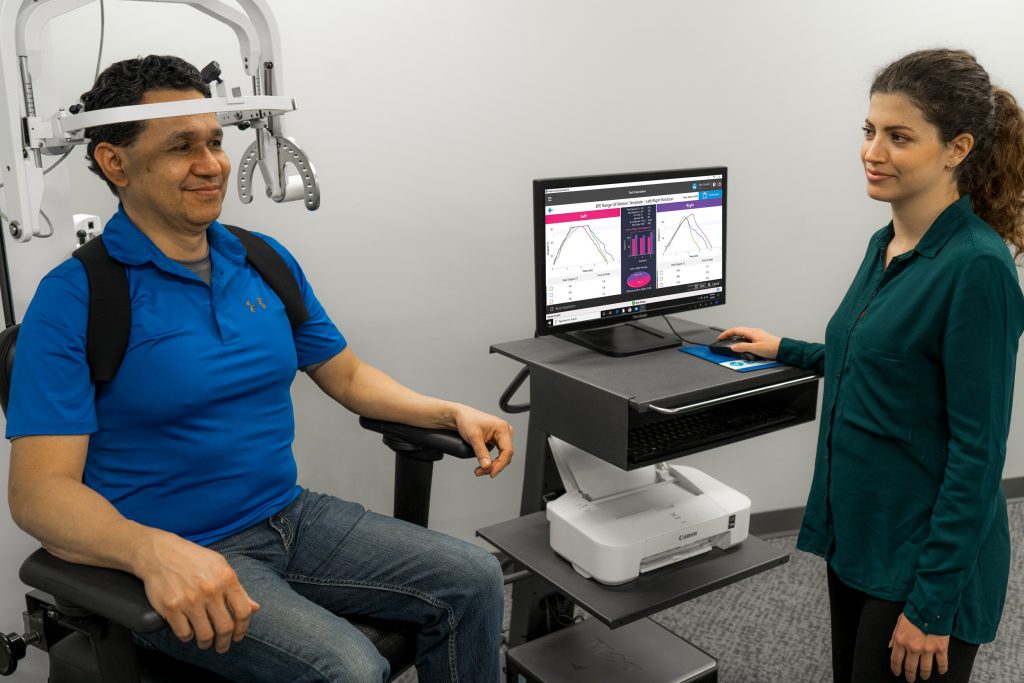
With the Multi-Cervical Unit (MCU), clinicians can evaluate and strengthen the neck muscles through controlled cervical spine exercises. The MCU can help clinicians restore range of motion in the neck and support progressive, evidence-based neck strengthening as symptoms allow.
Just as important for documentation. MCU’s reports can clearly show objective data captured over the span of treatment, helping clinicians communicate change over time and support clinical decision-making.
Evidence-Based Treatment Approaches for WAD
Treatment for WAD emphasizes early active care and individualized approaches based on symptom severity and functional limitations. Treatment methods vary across WAD grades and recovery phases.
Early Active Care Methods
For WAD Grades I-II, research supports early movement and an “act as usual” approach. This includes:
- Gentle active range of motion exercises: Begin within 24-72 hours when tolerated
- Gradual return to normal activities: Avoid prolonged rest or immobilization
- Education and reassurance: Understanding normal recovery patterns reduces anxiety
- Pain management: Short-term use of appropriate medications when necessary
Multiple Treatment Methods for Persistent Symptoms
When symptoms persist beyond the acute phase (typically 2-4 weeks), a treatment approach becomes necessary:
- Manual therapy: Skilled mobilization and manipulation techniques
- Therapeutic exercise: Progressive strengthening and flexibility programs
- Patient education: Pain science education and self-management strategies
- Psychological support: Addressing fear-avoidance behaviors and coping strategies
For clinics that want more evidence-based exercises during cervical rehabilitation, systems like the Multi-Cervical Unit (MCU) can support controlled neck strengthening and help clinicians document change over time. The MCU is positioned to address neck strength and range of motion to help reduce symptoms commonly associated with whiplash, including neck pain and vertigo, when used as part of an appropriate plan of care.
Medication Management
Medication use in WAD should be targeted and time-limited:
- Acute phase: NSAIDs or acetaminophen for pain and inflammation
- Muscle relaxants: Short-term use for severe muscle spasms
- Avoid prolonged opioid use: Risk of dependency with limited long-term benefits
- Adjuvant medications: For neuropathic symptoms when present
Specialist Care and Advanced Interventions
Referral to specialists may be appropriate when:
- Symptoms persist beyond 6-12 weeks despite appropriate treatment
- Neurological symptoms worsen or fail to improve
- Significant functional limitations affect work or daily activities
- Psychological factors significantly impact recovery
Recovery Timelines by Grade
Recovery expectations vary by WAD grade:
- Grade I: Most people recover within 2-6 weeks
- Grade II: Recovery typically occurs within 6-12 weeks with appropriate treatment
- Grade III: May require 3-6 months or longer for optimal recovery
- Grade IV: Extended recovery period often exceeding 6-12 months
Treatment for Long-Term WAD Symptoms
Clinicians treating chronic or long-term Whiplash Associated Disorder can get clinical research, practical advice from clinic owners, and real-world case studies in our free e-book: Don’t Just Manage Neck Pain, Fix It for Good.
Final Thoughts
Whiplash Associated Disorder is difficult to measure and communicate clearly over time. Using structured classification, active care, and objective tracking helps clinicians move toward more consistent, defensible outcomes. When paired with tools that quantify strength and range of motion, WAD management becomes more measurable, repeatable, and easier to support across the full episode of care.
For individuals with persistent WAD symptoms affecting work capacity, specialized functional assessments may be recommended as part of the recovery process. When WAD symptoms impact occupational performance, healthcare providers may refer patients for comprehensive functional capacity evaluations to guide safe return-to-work planning. In our partner clinics, we often pair those objective findings with targeted cervical rehabilitation using the Multi-Cervical Unit to help guide safe activity progression and workplace accommodations.
