Carpal tunnel diagnosis often requires an in-depth examination of the client’s symptoms, ergonomics, and other telling clinical data.
In a previous post, I discussed some of the popular rehab techniques for carpal tunnel syndrome (CTS). This companion piece will examine a few diagnostic considerations that rehab professionals should consider when working with a patient who suffers from CTS.
Carpal tunnel syndrome can often be confused with other common conditions of the wrist and hand. Therefore, whether you’re seeing a patient with CTS symptoms via direct access or through a referral from another healthcare provider, you need to be sure you have established a clear diagnosis before proceeding with treatment.
Differential Diagnosis for Nerve Injuries of the Wrist and Hand
When someone complains of nerve symptoms in the hand, the clinician’s mind should immediately jump to a few main conditions.
Namely, the shortlist for diagnoses related to nerve pain in the hand usually includes the following:
- Carpal tunnel syndrome
- Ulnar nerve entrapment
- Cervical radiculopathies
Of course, other issues must be ruled out as well, but these three are often the ones that bear the closest consideration in this area.
The clinician can often be led toward a diagnosis of carpal tunnel syndrome by taking a thorough history and selecting the tests that provide the most compelling data.

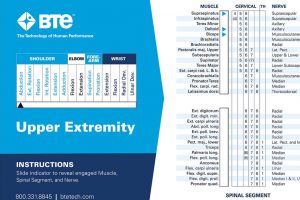
Quick Reference Tool for Innervation
A handy tool to help you recall which nerve innervates which muscle group involved in a particular movement is the Muscle Joint Action Guide (MJAG). The MJAG is a hand-held reference card that can help you identify and treat nerve damage. For example, your patient shows extreme weakness performing a certain muscle movement, use this cheat sheet to see which nerve controls it. And it works the other way around. If a patient walks in with diagnosed nerve damage, the Muscle Joint Action Guide will show you which muscle groups and joint-specific movements it affects. This information could show you a starting point in your treatment plan.
Carpal Tunnel Diagnosis: Patient History and Demographics
Often, patients with Carpal Tunnel Syndrome spend eight or more hours a day working with their hands. For this reason, we see many office professionals, who type for the majority of the day, presenting with this ailment. Additionally, CTS is more common in women and middle-aged adults.1
Of course, anyone can be affected by Carpal Tunnel Syndrome. A thorough examination is always needed to rule out other conditions and to rule in CTS.
Carpal Tunnel Diagnostic Tests and Examination
One of the most well-known special tests for CTS is Phalen’s sign. This test places the wrists in end-range flexion, fully compressing the contents of the carpal tunnel. In patients with severe symptoms, this test is likely to provoke the “classic” symptoms of lateral hand pain, numbness, and / or weakness.2 The reverse Phalen’s and Scratch Collapse tests are also quick and easy diagnostic tests which can provide more insight into the condition (although the results from these tests should be interpreted with caution and alongside all other clinical data).3,4
Wrist palpation is another effective way to identify any tissue restrictions or issues that may have led to the CTS symptoms.5 Palpation usually goes hand in hand with manual muscle testing and range of motion measurements, each of which can provide meaningful clinical data.
Also, there are a few other special tests that have stood the test of time for this condition, such as Tinel’s sign. Tinel’s sign involves tapping directly on the carpal tunnel to provoke the patient’s nerve pain. However, this test has low sensitivity.6
Combining some of the best research on diagnostic options for issues affecting the wrist and hand, the Clinical Prediction Rules for CTS may provide an expeditious way to arrive at a likely diagnosis of the condition.7 The CTS Clinical Prediction Rule looks at age, sensation, subjective symptom reports, wrist ratio, and ability to shake hands with another person. These measures offer promise for rapidly and accurately diagnosing CTS. That being said, this Clinical Prediction Rule is not currently recommended for clinical practice, as it has yet to be validated.
Differentiating Between Common Conditions of the Hand and Wrist
Taking into account the patient history, ergonomic considerations, and any other relevant clinical data gleaned from the examination, one can be reasonably certain that they’ve identified a case of CTS.
However, it is still valuable to rule out other similar conditions when appropriate.
Cervical radiculopathies can be tentatively diagnosed with a cluster of tests. Specifically, one cluster for this condition includes a positive cervical distraction test, a positive Spurling’s test, and a positive upper limb tension test. When considered along with symptoms and history consistent with cervical radiculopathy, this indicates that the patient likely has said condition. Likewise, negative results for all of these tests, while not enough evidence on their own to rule out the condition, can indicate that a cervical radiculopathy is not present.8
When it comes to ruling out ulnar nerve entrapment, we should first look to the patient’s chief complaint. Ulnar nerve entrapment typically results in symptoms on the medial side of the hand, rather than the lateral. However, if the symptoms are vague, there are a few key tests that can help to rule out ulnar nerve involvement such as Froment’s sign and the Ulnar Nerve Tension Test.9,10
If all of this information above indicates a carpal tunnel diagnosis, the clinician can then proceed with a research-backed treatment plan for managing the condition conservatively.
Summary
Carpal tunnel syndrome is an incredibly common condition for which we have a number of valuable tests and diagnostic tools. However, we need to be certain that we have correctly diagnosed the condition before we initiate treatment. This will often require an in-depth examination of the client’s symptoms, ergonomics, and other telling clinical data.
Naturally, once we’re reasonably certain that we’re dealing with a case of carpal tunnel syndrome, the next logical question is: “how do we treat it?” For the answer to this question, be sure to check out my companion piece on carpal tunnel syndrome.
Bennett Richardson, PT, DPT, CSCS
Bennett Richardson, PT, DPT, CSCS is a physical therapist and writer. He is the owner of Richardson PT LLC, a mobile, cash-based physical therapy service out of Pittsburgh, PA. Ben is passionate about many health-related topics including weight loss and athletic performance. To get in touch with Ben, visit www.richardsonpt.com
Works Cited
- Aroori, S., & Spence, R. A. (2008). Carpal tunnel syndrome. The Ulster medical journal, 77(1), 6–17.
- Cunha, T. A. L., Oliveira, O. M., & Ribeiro, M. B. (2020). PHALEN TEST POSITIVATION TIME AND ITS CORRELATION WITH ELECTRONEUROMYOGRAPHY. Acta ortopedica brasileira, 28(3), 114–116. https://doi.org/10.1590/1413-785220202803225744
- Cao, J., Jia, T., Lao, J., Liu, A., & Rui, J. (2022). Evaluation of different physical examination methods for the diagnosis of carpal tunnel syndrome. World Academy of Sciences Journal, 4, 33. https://doi.org/10.3892/wasj.2022.168
- Huynh, Minh N. Q. BSc*; Karir, Aneesh BHSc*; Bennett, Alexandria MSc*,†. Scratch Collapse Test for Carpal Tunnel Syndrome: A Systematic Review and Meta-analysis. Plastic and Reconstructive Surgery – Global Open 6(9):p e1933, September 2018. | DOI: 10.1097/GOX.0000000000001933
- Sucher BM. Palpatory diagnosis and manipulative management of carpal tunnel syndrome. J Am Osteopath Assoc. 1994 Aug;94(8):647-63. PMID: 7960973.
- Wiesman, I. M., Novak, C. B., Mackinnon, S. E., & Winograd, J. M. (2003). Sensitivity and specificity of clinical testing for carpal tunnel syndrome. The Canadian journal of plastic surgery = Journal canadien de chirurgie plastique, 11(2), 70–72. https://doi.org/10.1177/229255030301100205
- Wainner RS, Fritz JM, Irrgang JJ, Delitto A, Allison S, Boninger ML. Development of a clinical prediction rule for the diagnosis of carpal tunnel syndrome. Arch Phys Med Rehabil. 2005 Apr;86(4):609-18. doi: 10.1016/j.apmr.2004.11.008. PMID: 15827908.
- Kang, K. C., Lee, H. S., & Lee, J. H. (2020). Cervical Radiculopathy Focus on Characteristics and Differential Diagnosis. Asian spine journal, 14(6), 921–930. https://doi.org/10.31616/asj.2020.0647
- Cloete, D., & Lahri, S. (2019). Ulnar Nerve Injury and Froment’s Test: A Case Report. Cureus, 11(12), e6335. https://doi.org/10.7759/cureus.6335
- Nicole Manvell, Joshua J. Manvell, Suzanne J. Snodgrass, Susan A. Reid, Tension of the Ulnar, Median, and Radial Nerves During Ulnar Nerve Neurodynamic Testing: Observational Cadaveric Study, Physical Therapy, Volume 95, Issue 6, 1 June 2015, Pages 891–900, https://doi.org/10.2522/ptj.20130536